
A new paper from the Conboy lab at UC Berkeley, first-authored by Joana Marie C. Cruz and published in Aging Cell, deserves the attention of anyone who works with therapeutic plasma exchange. Before anything else, the vocabulary. What the researchers call plasma dilution, or neutral blood exchange (NBE), is therapeutic plasma exchange (TPE). It is the same procedure we perform at Global Apheresis, written in the language of a research lab: replace roughly half of the plasma with a saline and albumin solution, and you have reset the fluid every cell in the body is bathed in.
The study's headline is about aged hearts recovering from a heart attack, and that result is strong on its own. But the finding I want to lead with is quieter. The old mice who never had a heart attack, and received the plasma exchange anyway, finished the study stronger and with more endurance than when they started. That is the detail I think patients should understand, and I will come back to it.
For anyone who has followed this lab, the direction of these results will feel familiar. Their 2020 work showed that a single dilution of old plasma restored repair across brain, liver, and muscle. What is new here is the organ. Cruz and colleagues took the plasma exchange paradigm into the cardiovascular system, and did it under conditions that resemble how a heart attack actually lands in an older adult.
How the Study Was Built
The animals were C57BL/6 mice aged 18 to 22 months, which corresponds roughly to a human past sixty, the age window where the risk of a myocardial infarction climbs sharply. The investigators sorted them into four arms: a sham surgery group, a sham group that also received NBE, a group given ischemia-reperfusion (I/R) injury alone, and a group given I/R injury followed by NBE. The injury itself was produced by clamping the left anterior descending coronary artery for thirty minutes and then restoring flow, a controlled and reproducible heart attack.
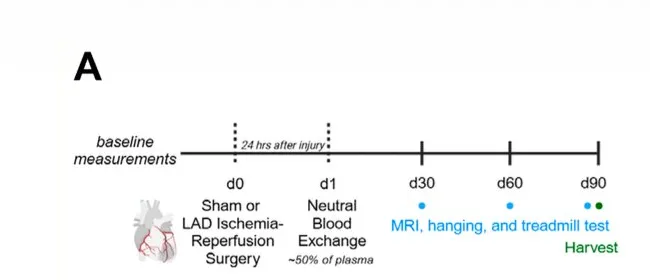
The timing is the part I would underline for any clinician. When a person has a heart attack, everything hinges on reopening the vessel fast: catheterization, a stent, minutes that matter. Nothing in this paper argues with that, and nothing here substitutes for it. The question Cruz and colleagues asked sits in the hours after that emergency work is done. Once flow is restored, is there anything worth doing to the body as a whole? They performed the plasma exchange a full day after the injury, past the acute ischemic insult, past reperfusion, but ahead of the inflammatory and scarring cascade that really gets going over the next several days. In the mice, intervening in that window changed the trajectory.
What Changed in the Injured Hearts
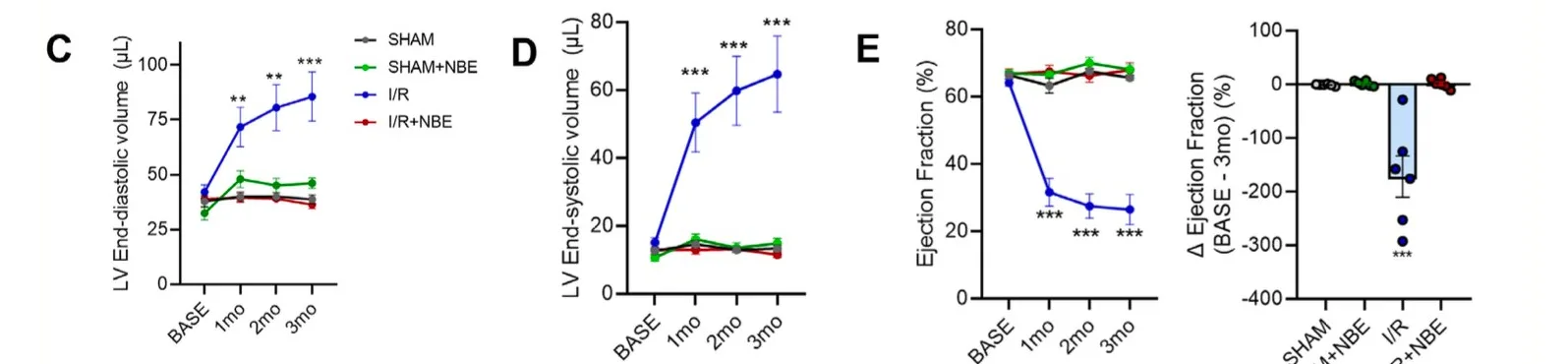
On serial MRI, the injured hearts that received NBE held onto their left-ventricular volumes and ejection fraction, statistically indistinguishable from the sham animals. The injured hearts that got nothing followed the familiar downhill path: progressive chamber dilation and falling ejection fraction across the three months. In plain terms, the treatment headed off the remodeling process that turns a heart attack into heart failure.
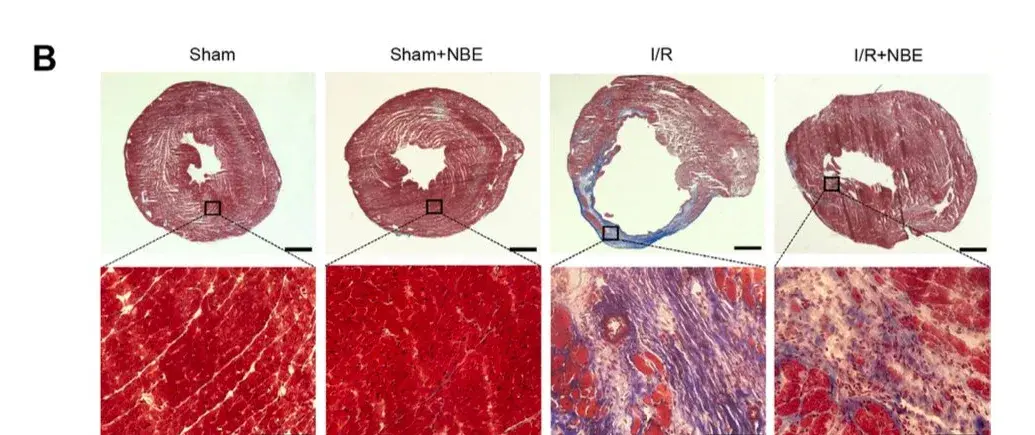
The tissue told the same story. At three months, the injured-plus-treated hearts had thicker walls at the infarct, smaller damaged areas, more surviving heart muscle, and noticeably less scarring on trichrome staining, with several pro-fibrotic proteins turned down on Western blot. Earlier, at day 5, those same hearts showed fewer infiltrating immune cells, fewer activated fibroblasts, fewer dying heart-muscle cells, and fewer senescent cells around the injury's edge. Inflammation, cell death, and cellular aging all bent in the favorable direction at once.
One result deserves special mention because of how stubborn the underlying problem is. Adult heart-muscle cells are famously poor at dividing again after they are damaged, which is a large part of why the heart recovers so badly compared with, say, the liver. Yet the treated hearts carried significantly more Ki67-positive cardiomyocytes in and around the infarct, a marker of cells re-entering the cell cycle. That hints the plasma exchange did not just quiet the damage. It nudged the environment toward something closer to genuine repair.
The Part I Keep Coming Back To
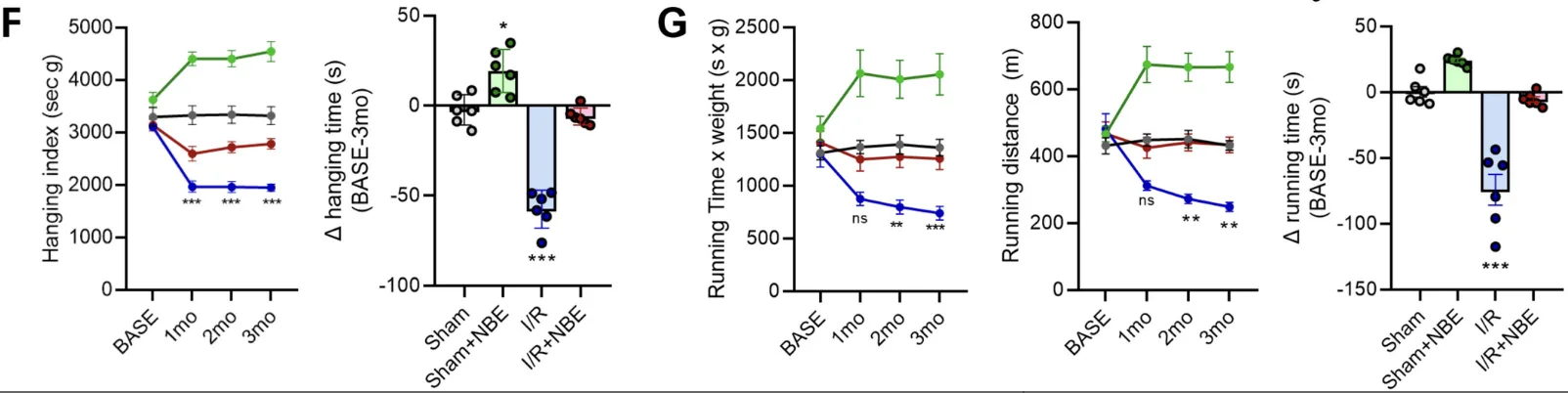
Now the finding that opened this piece. Grip strength and running distance both fell hard in the injured, untreated mice, each dropping by more than half from baseline over three months. The injured mice who received the plasma exchange largely held their baseline, reaching levels comparable to the uninjured shams. That contrast is impressive on its own.
But look at the group that never had a heart attack at all. The healthy old mice who received only the plasma exchange improved their hanging index by roughly 40% over the same three months and increased their treadmill endurance along with it, while the untreated healthy controls stayed flat. No injury to recover from. Just the treatment, and they finished stronger and lasted longer than they had at the start.
Plasma exchange improved physical function in aged animals with no disease and no injury at all. They finished stronger than they started.
That is the sentence I would want a patient to hold onto, because it maps onto why most people actually come to see us. They are not recovering from a cardiac event. They want to move better, hold their strength, and keep doing the things that make the later decades worth having. Improved performance in aging animals independent of any illness lands squarely on that preventive use case, and it is consistent with the broader rejuvenation literature.
We hear echoes of this from patients in the same age range: reports of better stamina and strength after treatment, including personal records set on the rowing machine. Those accounts are anecdotal, but they run in the same direction as the animal data, and that kind of alignment is what makes me watch this work closely.
What Is Actually Doing the Work?
The more interesting question is why any of this happens, and here the paper leaves room to think. I see two mechanisms that are not mutually exclusive.
The first is a reset of the aged milieu. The lab's prior work frames NBE as returning the systemic signaling environment to a pro-regenerative state simply by diluting old plasma. On that view, the plasma exchange does not target the heart at all. It lowers the age-associated factors that suppress repair everywhere in the body, and the heart benefits as one tissue among many.
The second is the removal of the post-heart-attack inflammatory surge. A heart attack sets off a wave of inflammation. Some of that acute response is necessary and useful for clearing dead tissue. But in an aged system the response often overshoots, and it is that overcompensation that drives excess fibrosis and worse function. A plasma exchange performed 24 hours in, right before the cascade peaks, could dilute the pro-inflammatory and pro-fibrotic signals before they lock in a large scar. The paper's own data fit this reading: lower inflammatory markers, fewer activated fibroblasts, and reduced fibrotic signaling, with the candidate pathways the authors highlight, JAK/STAT and TGF-β, sitting right at the interface between inflammation and scarring.
The proteomics sharpen this further. When the authors profiled newly made heart proteins, the plasma exchange only ever turned things down, never up. Twelve proteins that the heart attack had driven up, mostly inflammatory and growth-signaling factors, were brought back toward normal, and nothing was newly overproduced. The treatment was subtracting excess, not adding a stimulus. And it did so with a light touch: NBE attenuated TGF-β signaling without shutting it off. That distinction matters, because some of that signaling is exactly what a healing heart needs. This is the version of the second mechanism I find most convincing. Not wiping out the post-heart-attack response, but trimming its overshoot while leaving the useful part intact. That fits the basic clinical intuition that acute inflammation after an injury is not the enemy; the excess is.
Here is the tell that at least part of the effect is the first mechanism. The healthy animals had no heart attack, so there was no post-MI inflammatory surge to remove. Their gains in strength and endurance have to come from somewhere else, and the most parsimonious candidate is the milieu reset. That alone argues the benefit is not only about damping an injury response.
My read is that it is a combination. In the injured animals the plasma exchange is likely doing both at once: resetting the aged background environment toward repair, and, by the timing, diluting the overcompensating post-MI inflammatory and fibrotic signals before they scar the heart. Teasing those apart is the next experiment, and it matters. It would tell us how tightly the timing of a treatment needs to track an acute event, versus how much of the benefit comes simply from resetting the milieu on a longevity schedule.
Where This Sits in the Larger Arc
For more than twenty years the Conboy lab has been building the argument that much of what we file under intrinsic aging is actually driven by the systemic environment, the mix of proteins and signals a tissue is bathed in. Their 2020 paper (Mehdipour et al., Aging) made the cleanest version of that case: diluting old plasma, without adding anything young back in, was enough to restore maintenance and repair across three germ layers.
The Cruz paper extends that logic to the heart, under acute-injury conditions, with a delayed-treatment design that resembles real clinical timing far more than most animal work does. Earlier plasma exchange studies showed benefit in muscle, liver, and brain. This one adds the cardiovascular system, and specifically, recovery from the single event that kills more people worldwide than any other.
Read alongside the human work, including the finding that old-plasma dilution can lower measured biological age (Kim et al., GeroScience, 2022), it strengthens a case we have been building for years. Therapeutic plasma exchange may do more than strip out cholesterol and inflammatory mediators. It may help reset the signaling environment the heart muscle itself lives in, pushing cells toward repair instead of scar.
Why I'm Watching This Closely
The procedure in this study is, in essence, what we perform at Global Apheresis, where I serve as Associate Medical Director. Every therapeutic plasma exchange resets that systemic milieu. For years we have had animal evidence that doing so supports muscle, liver, and brain in aging tissue. The Cruz paper now puts the heart, the organ most responsible for killing older adults, on that same list, and adds hard performance numbers in animals that were never sick to begin with.
Dr. Dobri Kiprov, with whom I work at Global Apheresis, has co-authored plasma dilution research with the Conboy group, and our practice keeps a direct line to the UC Berkeley lab behind this work. This is still animal data, and I will not dress it up as more than that. But it is the kind of result that tells you where the translational work is heading, and when the next step is taken, I expect us to be part of that conversation.
Allen P. Green, M.D., is Board-Certified in Clinical Pathology and serves as Associate Medical Director at Global Apheresis in Mill Valley, California. He writes on plasma exchange, environmental medicine, and longevity research.
To discuss whether therapeutic plasma exchange is appropriate for your situation, schedule a complimentary Discovery Call. Most consultations are conducted via telehealth.